

Abstract
Introduction:
Transfusion of blood products can be associated with a wide variety of complications ranging in level of severity. The most lethal of these are Transfusion-Associated Circulatory Overload (TACO) and Transfusion-Related Acute Lung injury (TRALI). Over the five year period from 2012-2016, TRALI was the leading cause of transfusion-associated fatalities, closely followed by TACO. However, the incidence of these potentially lethal transfusion reactions in the pediatric population is not well known. Our objective is to describe the incidence of these transfusion reactions in pediatric patients and describe their associated morbidity and mortality.
Materials/Methods:
We used the Pediatric Health Information System (PHIS), an electronic database of children's hospitals in the USA. Data was obtained from 45 children's hospitals in 2005-2015 for patients ≤ 21 years of age who received transfusion of packed red blood cells, platelets, whole blood, coagulation factors, other serum and exchange transfusion. From this group of patients, we then identified patients who developed TRALI and TACO. Patients were identified by ICD9 codes for transfusion of various blood products and related adverse events. We abstracted data on demographics, medication use, length of stay (LOS), hospital charges and mortality.
Results:
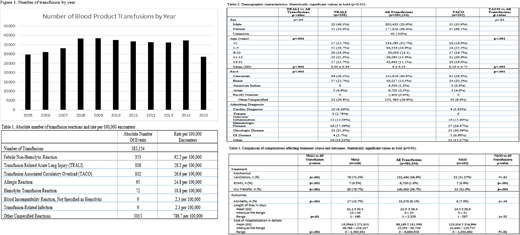
During the study period, 383,154 inpatient encounters in which patients received a blood product transfusion were identified. Overall the number of blood product transfusions has remained stable (Figure 1). There were 982 transfusion reactions per 100,000 hospital encounters over this period and the incidence rates of each type of transfusion reaction are described in Table 1. In our patient cohort, 108 cases of TRALI and 102 cases of TACO were identified. Cohorts were similar with regards to gender distribution. Distributions of age and race differed between the TRALI and TACO cohorts compared to the all transfusions cohort (Table 2). The morbidity, mortality and hospital charges of encounters complicated by TRALI and TACO are described in Table 3. In the TRALI cohort, a significantly greater number of patients required mechanical ventilation, ECMO or transfer to the ICU and had a greater increase in mortality in comparison to the all transfusion cohort. The TACO cohort had a significantly increased number of patients who required ECMO or ICU transfer compared to the all transfusions cohort. Length of stay was significantly greater for patients in the TRALI cohort compared to the all transfusions cohort. Patients diagnosed with either TRALI or TACO had significantly increased costs associated with hospitalization.
Conclusion:
Our study demonstrated that both TRALI and TACO are associated with an excess morbidity and mortality. However, the number of cases of TRALI and TACO in our study were fewer than what was expected based on previous studies. This indicates that TRALI and TACO are likely under-diagnosed and under-reported. Efforts should be made to increase awareness of recognizing and reporting of these transfusion reactions to improve the outcome of these potentially lethal complications.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal